/prod01/prodbucket01/media/durham-university/departments-/engineering/74202-5112X1676.jpg)
Bioengineering Research Group Projects
See below for some selected projects of the group.
Paediatric bone characteristics
/prod01/prodbucket01/media/durham-university/departments-/engineering/Borghi1.png)
Minimally invasive endoscopy assisted craniectomy
/prod01/prodbucket01/media/durham-university/departments-/engineering/Borghi3.png)
AI tool to aid with ophthalmology triage service
/prod01/prodbucket01/media/durham-university/departments-/engineering/Kafieh1-1000X575.png)
Brain and eye connectivity
/prod01/prodbucket01/media/durham-university/departments-/engineering/StProjDewhurst-500X342.png)
Flow asymmetry in pulmonary arteries
/prod01/prodbucket01/media/durham-university/departments-/engineering/StProjGbinigie.jpeg)
Characterisation of paediatric cranial bone
The macrostructure of the cranial bone evolves from one layered structure in childhood to three-layered structure in adults, consisting of two external cortical tables and a central diploe layer. Works in the literature have shown that surgical outcomes are related to bone micro-architecture rather than age and bone mechanical response can be measured by means of standardised methods of mechanical characterisation. I plan to use a combination of mechanical testing protocols (indentation, three-point-bending), high resolution imaging (microCT) and numerical modelling techniques (µFEA) to assess the variation in mechanical characteristics and response with age in paediatric bone to understand why.

Micro-CT images (A) 1-layered structure and (B) 3-layered parietal bones; C) Changes in head shape (cephalic index, CI – a clinical indicator of head shape) for bones classified as one or three layers. *p < 0.05; D) Relationship between change in CI and patient age at the time of spring insertion. Two 7.2-month-old patients (1 and 2) show substantially different outcomes.

Three point bending (on the left) and reference point indentation (on the right) tests of paediatric calvarial bone.
Minimally invasive endoscopy assisted craniectomy
Metopic Craniosynostosis (MC) is a complex craniofacial anomaly where the forehead suture (metopic) fuses prematurely and cause abnormal forehead development. Surgical treatment involves extensive skull reshaping, usually during the first year of life. Recently, minimally invasive endoscopy assisted craniectomy (ESC) - involving endoscopic resection of the synostosic suture via a small frontal incision - has been adopted worldwide for the treatment of MC. ESC in conjunction with the application of cranial orthosis – helmet – (ESCH) has shown very promising results both in terms of aesthetic and functional improvement Early minimally invasive surgical correction is recommended; however it is not well understood how age, type of craniosynostosis, surgical technique, and post-operative orthosis implementation affect patient cosmetic outcomes. The aim of this project is to produce a validated numerical model for the outcome prediction of ESCH to understand and optimise the treatment strategy as well helmet design.

A baby who received ESCH (on the left - https://www.flickr.com/photos/150hp/6270854045) and numerical simulation of helmet therapy (on the right)
AI tool to aid with Ophthalmology triage service
Due to the severe shortage of consultant ophthalmologists in the UK, patients are currently not being seen in a timely manner, with obvious risks to patient eyesight. In collaboration with UKBB, Newcastle Hospital Trust, and County Durham Trust, a database of images will be collected and their changes over time will be used in an AI tool to identify the patients at most risk of disease progression. 
Artificial Intelligence can be used in different medical imaging applications by facilitating early and precise diagnosis, effective treatment, and accurately evaluated follow-ups.
Brain and eye connectivity
Eye is known as a mirror to brain, with physical connections in-between. This is a great opportunity to study less invasive images of the eye to determine the changes of the brain. The currently available datasets of Iran and UKBB are great sources as input to AI methods. The expected output is neurological problems, the sate of the disease, or their severity, determined by standard methods like brain imaging.
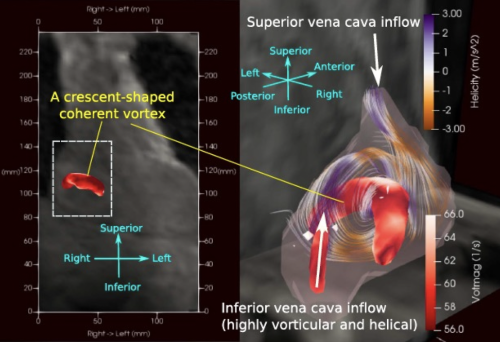
Coherent vortex flow structure in the right atrium
In healthy adults, the right atrium (RA) serves as a reservoir for the systemic flow return from the superior vena cava (SVC) and inferior vena cava (IVC), preparing the two flows to be transferred to the right ventricle (RV) and pulmonary circulation. This study aims to quantify the haemodynamics of the RA and the associated SVC and IVC inflows, which have not been fully understood to date. Approach: Eighteen adults with structurally normal hearts underwent 4D flow magnetic resonance imaging. The cardiac cycle was resolved to 20 temporal phases with a spatial resolution of 3 × 3 × 3 mm3. Analysis included objective visualisation of the flow structures in the RA identified by three different vortex identification criteria, kinetic energy (KE), enstrophy and dissipation. KE and helicity flux were also assessed in both caval veins. Main results: Vortex identification methods confirmed that in the majority of participants the blood flow from the caval veins filling the RA during ventricular systole is not chaotic, but rather forms an organised pattern of a single coherent forward turning vortex structure. Thirteen participants displayed a single vortex flow structure, four showed multiple vortices and one had a helical flow pattern without a clear vortex structure. A strong positive correlation exists between the flow KE and enstrophy density. Significance: This suggests that flow energy in the RA is mainly rotational, part of which is convected by the highly helical SVC and IVC inflows. Multiple vortices tend to be associated with higher dissipation rates in the central RA region due to turbulence. The rotational nature of the flow in the RA maintains KE better than non-rotational flow. RA flow characteristics are highly related to the helicity content in the caval veins, as well as the KE flux intensity. Lower caval helicity or IVC KE flux dominance tends to favour single vortex formation while the opposite tends to lead to multiple vortices or the rare helical flow patterns. Atria lacking single vortex flow are inclined to have a larger energy input from atrial contraction.
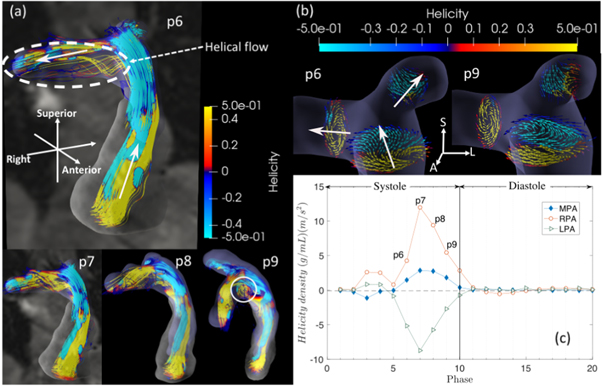
Asymmetric flow pattern in pulmonary arteries
We elucidate the asymmetric flow pattern and the haemodynamic quantity distributions and correlations in the pulmonary artery (PA) vasculature in healthy adults having structurally normal hearts, to provide reference on the flow characteristics in the PA and the right ventricle. Approach. Velocity data are acquired non-invasively from 18 healthy volunteers by 4D flow magnetic resonance imaging, resolved to 20 phases with spatial resolution 3 × 3 × 3 mm3. Interpolation is applied to improve the accuracy in quantifying haemodynamic quantities including kinetic energy, rotational energy, helicity and energy dissipation rate. These quantities are volumetrically normalised to remove size dependency, representing densities or local intensity. Main results. Flow asymmetry in the PA is quantified in terms of all the flow dynamic quantities and their correlations. The right PA has larger diameter and higher peak stroke velocity than the left PA. It also has the highest rotational energy intensity. Counter-rotating helical streams in the main PA appear to be associated with the unidirectional helical flow noticed in the left and the right PA near the peak systole. Significance. This study provides a fundamental basis of normal flow in the PA. It implies the validity to use these flow pattern-related quantitative measures to aid with the identification of abnormal PA flow non-invasively, specifically for detecting abnormalities in the pulmonary circulation and response to therapy, where haemodynamic flow is commonly characterised by increased vortical and helical formations.